



Creating a medical care experience that generates trust and gives value to people and buyers is not a quick solution, but it is the only way to reverse the descending spiral of high costs and bad results
Entrepreneurs like to say that the United States’s health system is “broken”, habitual just before explaining how they intend to solve it. I have a slightly different diagnosis.
The US health system is the gold standard. Our institutions and companies, ranging from 200 -year academic centers to new digital health companies, are clear world leaders in clinical experience, research, innovation and technology. Capabilities, the system is far from breaking.
What is broken is trust In the system, due to the obvious gap between what the system is capable and what real offers. Every day throughout the country, the people who drive fit world -class hospitals, but then to wait months for a primary care event. They deduce hundredths for medical care of each payment check, just to be told in the pharmacy that their recipe is not covered. While waiting for a state -of -the -art scan, they are given a clipboard and are asked to recapitulate their medical history.
This Whipsesw experience is not due to incompetence or poor infrastructure. It is the product of dysfunction between the two largest players in medical care: suppliers and insurers, two entities that have optimized their respective businesses, in opposition to each other, and inadvertently at the expense of people.
Historically, hospitals and health systems, including 200 -year AMC, have completely dedicated themselves to improving and saving lives. I do not say that they have lost sight of this, but even recent, margin tok a rear seat to the mission. However, with the consolidation of industry and the persistence of the service rate model, the hands of suppliers have been forced to maximize the volume of attention to the highest possible unit cost, which in turn has become a main driver of the cost of control.
This thrust of suppliers has caused an equal and opposite reaction of insurers. He thought that the industry has been villainized (rightly, in some cases) for a heavy approach to the management of use and prior authorization, insurers are simply doing what their main customs employers have hired them to do: administer. Insurers have very good Goths, not only by limiting attention, but also through the innovation of products that have created more levels and cost options for sponsors of the plan.
Meanwhile, medical care consumers (people!) They have set aside in the middle of this strip and loosen. Doctors and hospitals say they are patientAnd insurers say they are Centered member – But jargon is a dead raffle. Each side focuses on the half of the cake, and Neith is responsible for whole Person: The person who receives attention and Pay for attention, not to mention navigate everything in the middle.
I should not surprise that trust is fun. Only 56% of Americans trust their health insurer to act in their best interest. Even confidence in doctors, the good ones, has collapsed. In a surprising reversal of only four years ago, a huge 76% of people believe that hospitals care more about income than patient care.
| Loss of confidence in medical care suppliers | |
| Hospitals in the United States They focus mainly on … |
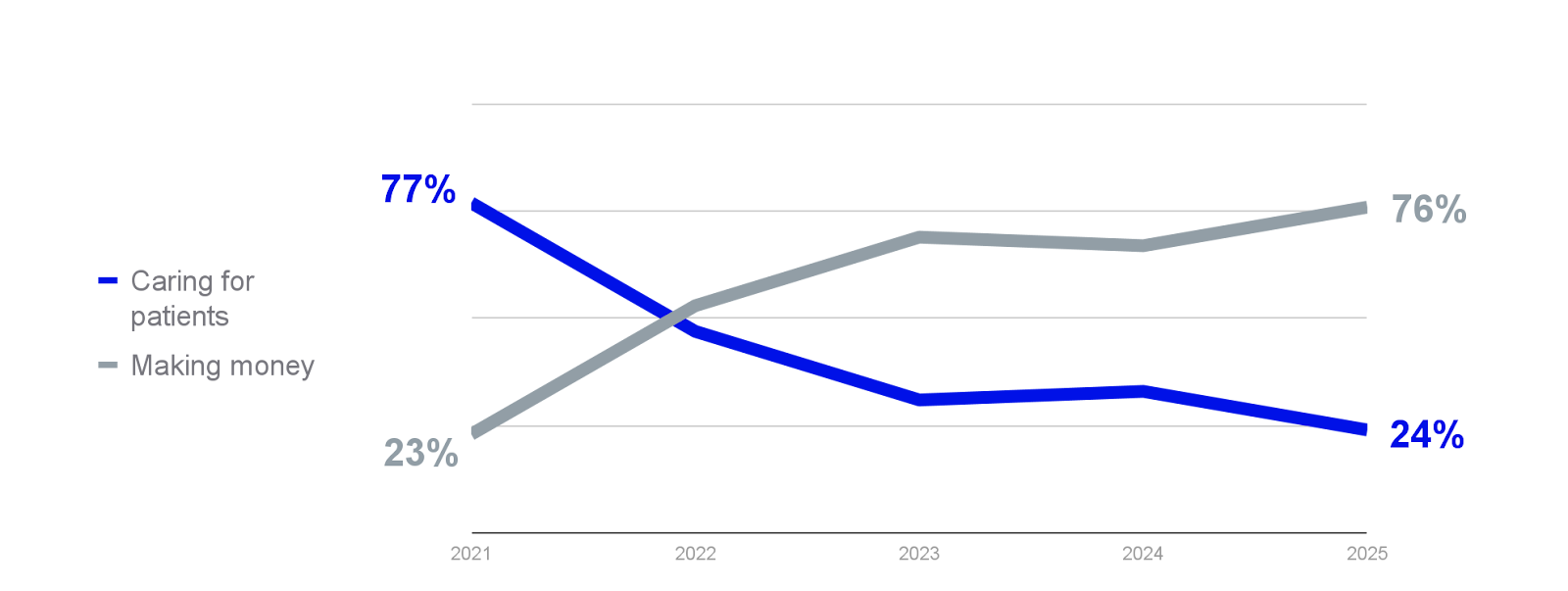 |
| ⏺ Take care of patients ⏺ earn money
Source: Jarrard/Chartis (2025) |
|
This trust deficit is the root cause of so many health problems. It is the reason why people disconnect, delay and omit attention, and end in the emergency room or for preventable problems. When a good part of the population falls in this cycle, as they have done, it ends with the status quo: costs of relieving and deteriorating the results that are dragging households, companies and the industry themselves.
There is no quick solution. Despite what my entrepreneurs could say, no solution or technology of a point (no, not even AI) can rebuild trust. The only way to reverse the descending spiral is to serve a modern experience that is really designed around the needs of people.
Prepare: Building that experience does not require reconstructing the entire system. But it requires a change of step. It is time for leaders and innovatives of the entire ecosystem to reinvent and redefine associations, care of people and payment models to create a new center of gravity in medical care, one that sits outside the traditional tool and insurance they offer. That is the solution, and this is what I think is seen:
People and buyers, together
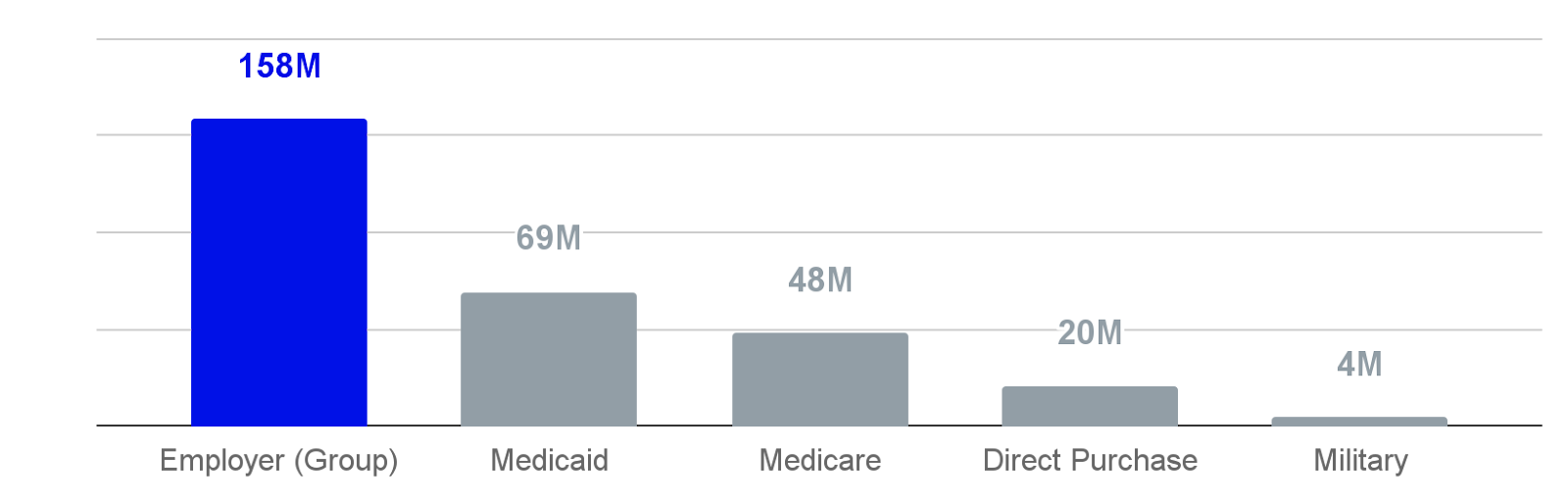
The group commercial insurance market can be the new center of gravity of Healthcare. Think about it: collectively, private employers and public sector organizations that make up the market represented the largest medical care buyers in the country, providing health insurance to almost 160 million Americans. Thanks to their scale and influence, thesis organizations are uniquely positioned to the real increase above the status quo and create an alternative to the dynamics of the supplier insurer.
| Health Insurance Coverage of the American populationSource: KFF (2023) | |
 |
In addition to the scale, the interests and incentives of the sponsors of the thesis plan are naturally aligned with those they cover. People (employees) and buyers (employers) want the same. Employees and their families want healthier days, with lower premiums and pocket expenses. Employers want a healthy, happy and productive workforce, while reducing their astronomical health spending, projected to increase 9% for private employers this year. In contrast to the zero sum game between suppliers and insurers, the best health results at lower cost are a mutual benefit for people and buyers.
Self -financed employers, who represent two thirds of the group market, and biased more important or especially important players, due to their purchasing power and their ability to cure the benefits and services for their workforce in which it is brought. Instead of trusting a single carrier, many self -financed employers contract directly with the main brick and mortar health systems (as in the model of Centers of Excellence), as well as the best service providers throughout the medical care ecosystem.
End -to -end integration (really)
The historical division between suppliers and insurers has fractured the health experience, but that is not the only guilty. In fact, the proliferation of points solutions, digital health applications and third -party service providers has exacerbated many of the cracks and weak points in the system. The “front doors” that claim to rationalize the experience of medical care for employees too often open to the same fragmented and confused landscape, if they lead anywhere.
Experience repair should begin with integration, and not just clinical integration. Yes, integrated care is important. Connect primary care with the health of behavior and specialized care, combining virtual experiences and in person, providing the access to access to the same data, are all the essential steps. But integration must go much further. The quality and clinical results are inseparable from the administrative, financial and logistics aspects of medical care that have long varied between suppliers and insurers.
People intuitively understand the relationship between their mental, physical and financial health, and need a reliable support system that addresses all dimensions together, through navigation, financial service and the other of another.
A modern version of value based on value
Value -based attention has seen a long leg as a solution to misaligned incentives that the rate forum model has created between suppliers and insurers. However, two decades of experiments directed by Medicare have mixed (some would say that disappointing) results. But those who ask for the end of the value based on the value are overlooking the without exploiting potential for the alternative payment and provision of attention in the commercial market always important.
The value of health, as a concept and practice, is relatively new in commercial space. The agreements based on the value between the sponsors of the Health Plan and their medical care partners have greatly limited to the payment models for performance and the payments grouped for specific clinical services (as with the centers of excellence). While some of these specific solutions provide savings, measuring ROI has been more an art than a science. Specifically, the lack of integration described the suppliers of multiple voltage services of integration, as well as the clinical and non -clinical services have made it difficult for the sponsors of the plan to attribute the improved results or the cost savings to the specifications.
The new value -based association models are changing that. Contracts based on the value of thought can take many forms, the avant -garde in the commercial market is a shared savings model that encourages health service suppliers and insurers to join forces and boost the results that matter to people and Buyers, including experience, clinical quality and, most importantly, the total cost of care. It is not enough to have adequate partners and capabilities in place. The model must guarantee alignment and responsibility.
Conclusion: From the descending spiral to the steering wheel
When these pieces join in a medical care experience that gains people’s confidence, the spiral of high costs and bad results begin to be reversed. An easier and more integrated experience of people first drives commitment, which improves the results. The best experiences and results generate trust, which promotes greater commitment, etc. The possible effect of the steering wheel is activated: as people become healthier, they need less high cost, and are more resistant and productive, and that value is transmitted to the buyer.
Medical care is not broken. We do not need to disassemble or review the system. We only need to participate in a better training so that the best of the system works for people, not against them.
Owen Tripp is the co -founder and CEO of Health includedA personalized medical care company in one that is associated with employers and public sector organizations on value based on value.
]